


 Sign Out
Sign Out

Switching from other antipsychotics: It is recommended that gradual discontinuation of the previous treatment should be done when risperidone therapy is initiated. The period of overlapping antipsychotic administration should be minimized. If necessary, when switching patients from depot antipsychotics, initiate risperidone therapy in place of the next scheduled injection. The need for continuing existing anti-Parkinson drugs should be reevaluated periodically.
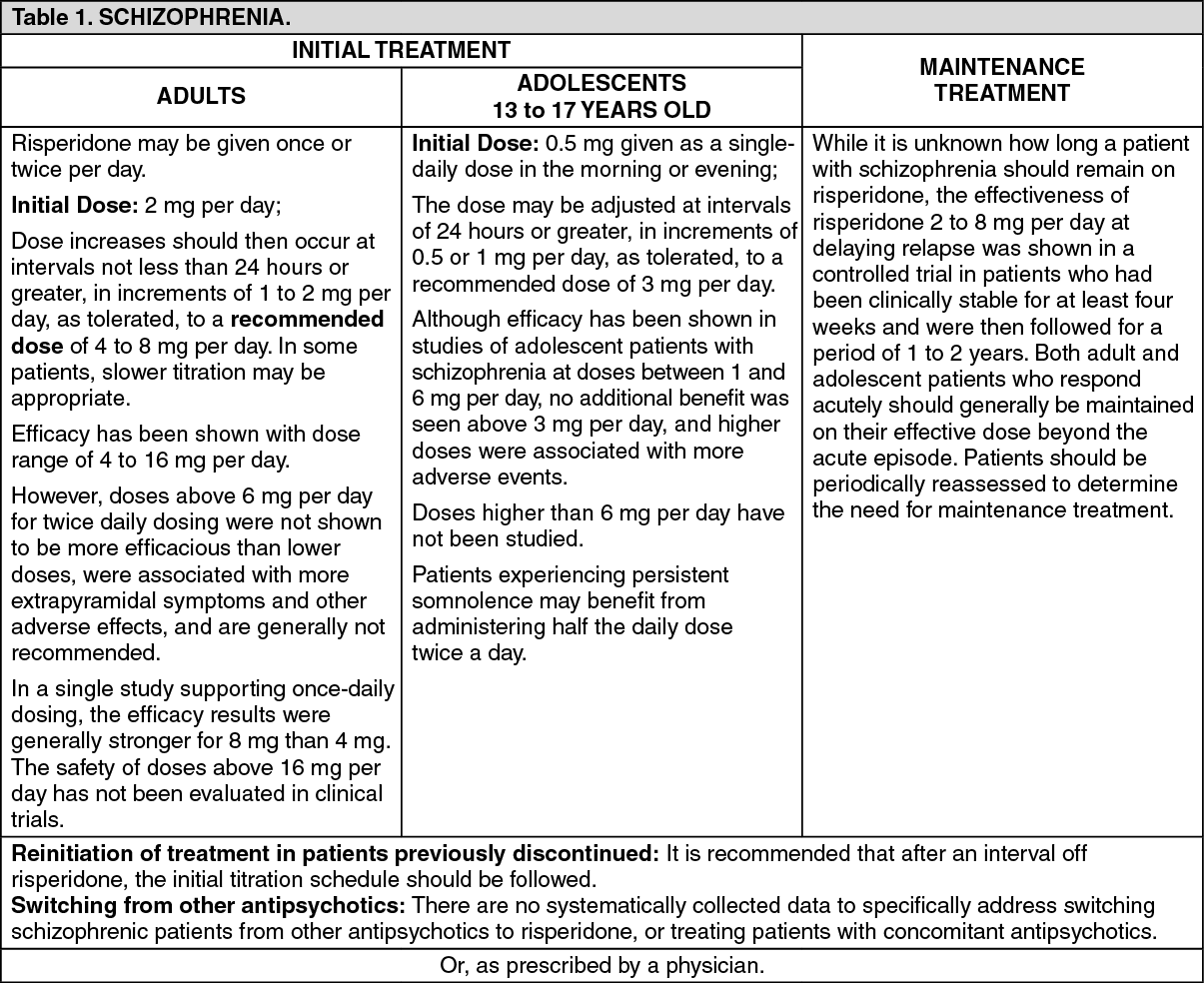
Recommended Oral Risperidone Dose: See Tables 1, 2 and 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image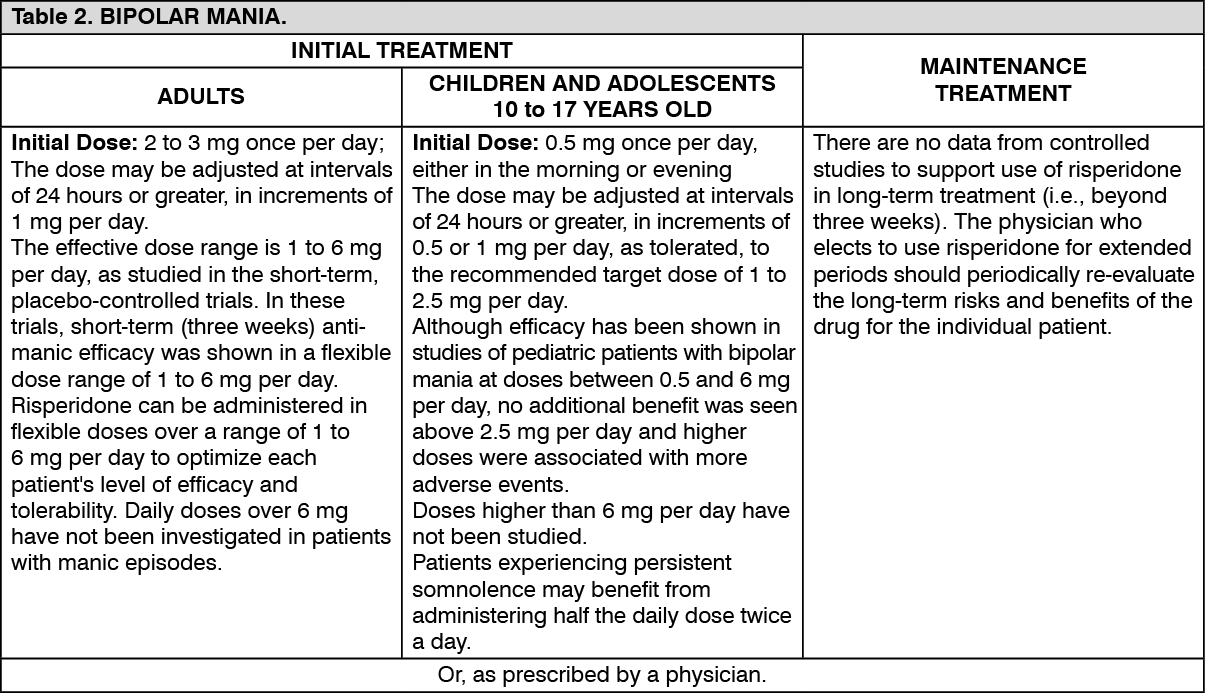 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image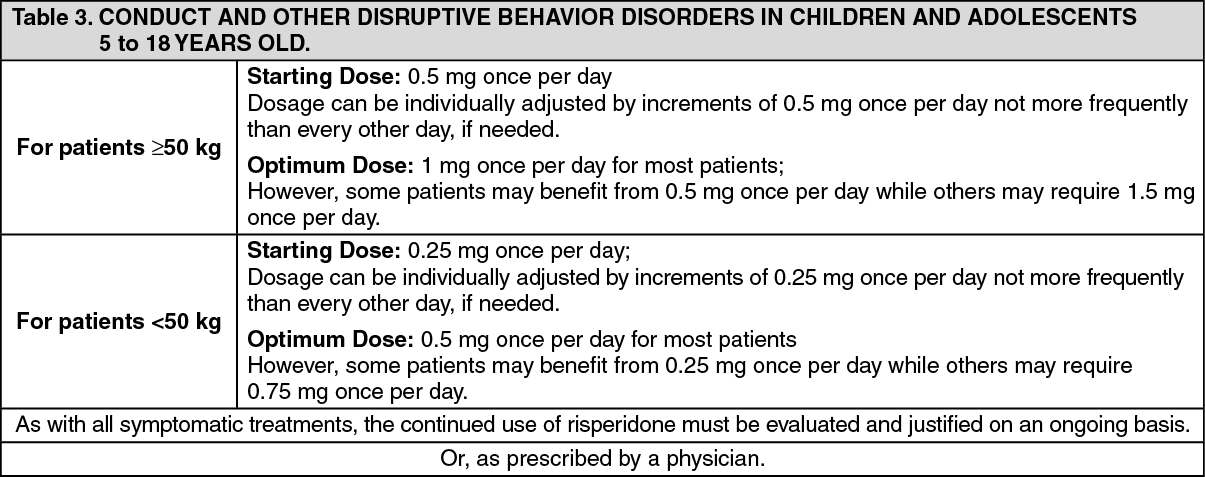 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIrritability Associated with Autistic Disorder in Children and Adolescents 5 to 16 years old: The dosage of risperidone should be individualized according to response and tolerability of the patient.
The total daily dose of risperidone can be administered once per day, or half the total daily dose can be administered twice per day.
Initial Dose: Patient Weight: <20 kg: 0.25 mg per day.
≥20 kg: 0.5 mg per day.
After a minimum of four days from treatment initiation, the dose may be increased to a recommended dose of 0.5 mg per day for patients <20 kg and 1 mg per day for patients ≥20 kg. This dose should be maintained for a minimum of 14 days.
In patients not achieving sufficient clinical response, dose increases may be considered at ≥2-week intervals in increments of 0.25 mg per day for patients <20 kg or 0.5 mg per day for patients ≥20 kg. The effective dose range is 0.5 to 3 mg per day. No dosing data are available for children who weigh less than 15 kg.
Once sufficient response has been achieved and maintained, consider gradually lowering the dose to achieve optimum balance of effectiveness and tolerance. The physician who elects to use risperidone for extended periods should periodically re-evaluate the long-term risks and benefits of the drug for the individual patient.
Patients experiencing persistent somnolence may benefit from a once per day dose administered at bedtime or administering half the daily dose twice per day, or a reduction of the dose.
As with all symptomatic treatments, the continued use of risperidone in children and adolescents with autism must be evaluated and justified on an ongoing basis.
Behavioral disturbances in patients with dementia: Physicians are advised to assess the risks and benefits of the use of risperidone in elderly patients with dementia of the Alzheimer type, taking into account risk predictors for stroke or existing cardiovascular comorbidities in the individual patient.
Discontinuation should be considered if signs and symptoms of cerebrovascular adverse events occur.
Initial Dose: 0.25 mg twice per day.
This dosage can be individually adjusted by increments of 0.25 mg twice per day, not more frequently than every other day, if needed. The optimum dose is 0.5 mg twice per day for most patients. Some patients, however, may benefit from doses up to 1 mg twice per day.
Periodic dosage adjustment (increase or decrease) or discontinuation of treatment should be considered because of the instability of the symptoms treated.
Once patients have reached their target dose, a once per day dosing regimen can be considered. As with all symptomatic treatments, the continued use of risperidone must be evaluated and justified on an on-going basis.
Special Population: Patients with severe renal (CLcr<30 mL/min) or hepatic impairment (10 to 15 points on Child Pugh System): Initial Dose: 0.5 mg twice per day.
The dose may be increased in increments of 0.5 mg or less administered twice per day. For doses above 1.5 mg twice per day, increase in intervals of one week or greater.
Elderly: The doses of risperidone should be adjusted slowly from a 0.25 mg twice per day starting dose to a maximum daily dose of 3 mg. Since the elimination of risperidone is somewhat slower in these patients, the potential for accumulation should be considered.
Patients prone to hypotension: Caution should be exercised in patients prone to hypotension and the use of lower starting doses of 0.25 to 0.5 mg twice per day should be considered.
Dose adjustment for specific drug interactions: When risperidone is concomitantly use with enzyme inducers (e.g., carbamazepine), the dose of risperidone should be increased up to double the patient's usual dose. It may be necessary to decrease the risperidone dose when enzyme inducers such as carbamazepine are discontinued. Similar effect may be expected with concomitant use of risperidone with other enzyme inducers (e.g., phenytoin, rifampicin, and phenobarbital).
When fluoxetine or paroxetine is concomitantly use with risperidone, the dose of risperidone should be reduced. The risperidone dose should not exceed 8 mg per day in adults when concomitantly used with these drugs. When initiating therapy, risperidone should be titrated slowly. It may be necessary to increase the risperidone dose when enzyme inhibitors such as fluoxetine or paroxetine are discontinued.
Or, as prescribed by a physician.